
FDA verleent De Novo Designation voor Adaptive Biotechnologies’ clonoSEQ Assay voor het opsporen en bewaken van minimale restziekten (MRD) bij patiënten met multipel myeloom en acute lymfoblastische leukemie
SEATTLE–(BUSINESS WIRE)–
clonoSEQ is een eersteklas NGS-assay en de eerste en enige FDA-goedgekeurde MRD-assay voor elke lymfoïde kanker
Adaptive Biotechnologies® kondigde vandaag aan dat de Amerikaanse Food and Drug Administration (FDA) De Novo designation voor de clonoSEQ® Assay heeft toegekend voor het opsporen en controleren van een minimale residuele ziekte (MRD) bij patiënten met multiple myeloom (MM) en B-cel acute lymfobe leukemie (ALL) met behulp van DNA uit het beenmerg van een patiënt. De goedkeuring van clonoSEQ markeert verschillende “primeurs” voor patiënten en voor de FDA.
FDA Grants De Novo Designation for Adaptive Biotechnologies’ clonoSEQ Assay to Detect and Monitor Minimal Residual Disease (MRD) in Patients with Multiple Myeloma and Acute Lymphoblastic Leukemia
SEATTLE–(BUSINESS WIRE)–
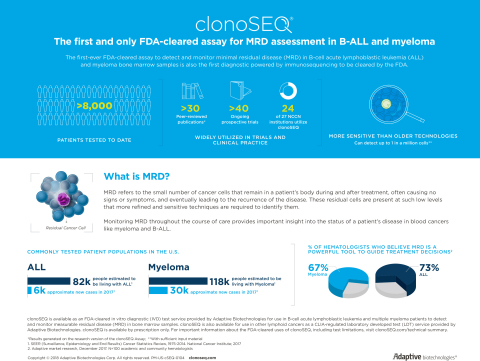
clonoSEQ is a first-in-class NGS assay and the first and only FDA-cleared MRD assay for any lymphoid cancer
Adaptive Biotechnologies® announced today that the U.S. Food and Drug Administration (FDA) has granted De Novo designation for the clonoSEQ® Assay to detect and monitor minimal residual disease (MRD) in patients with multiple myeloma (MM) and B-cell acute lymphoblastic leukemia (ALL) using DNA from a patient’s bone marrow sample. The clearance of clonoSEQ marks several “firsts” for patients and for the FDA. The clonoSEQ Assay represents a first-in-class MRD assay that uses next-generation sequencing (NGS) technology to assess disease burden, representing an important additional use of NGS in cancer. clonoSEQ is the first and only assay to be cleared by the FDA for MRD assessment in any lymphoid cancer and the first FDA-cleared diagnostic assay powered by immunosequencing. It is also a major milestone for Adaptive Biotechnologies as the first regulatory clearance for the company’s proprietary (NGS) platform for immune system profiling.
This press release features multimedia. View the full release here: https://www.businesswire.com/news/home/20180928005655/en/
Detecting Minimal Residual Disease in MM and ALL (Graphic: Business Wire)
MRD refers to the small number of cancer cells that can remain in a patient’s body after treatment, which often cause no signs or symptoms but eventually can lead to recurrence of the disease. These residual cells can be present at very low levels and require highly sensitive tests to identify them. Even very small amounts of MRD can have a profound effect on treatment success and patient outcomes. A test that can reliably determine the presence and amount of residual disease at very low levels can be used by physicians in conjunction with other clinical information to predict treatment outcomes, guide management decisions and improve patient care.
“MRD testing provides patients with real-time insights about their response to therapy or the depth of their remission, therefore the MMRF is deeply committed to this important advancement in patient care,” said Paul Giusti, president and chief executive officer, Multiple Myeloma Research Foundation (MMRF). “The sensitivity of the test is extremely important, as the number of cells remaining after treatment has been linked to patient outcomes. This clearance provides patients and physicians with access to a highly sensitive, standardized MRD test that can be an important tool in guiding treatment decisions.”
There are more than 200,000 MM and ALL patients living in the U.S., and more than 35,000 new cases are diagnosed each year. The clonoSEQ Assay uses NGS to precisely identify and monitor MRD in these patients throughout treatment and remission, with greater sensitivity than other technologies for any given amount of bone marrow sample.1 Detecting MRD with deep sensitivity can be clinically informative for the many patients being treated for these cancers.
“The FDA clearance of clonoSEQ is an important advance for patients with MM and ALL and for the oncologists who care for them. This milestone underscores the importance of MRD as a predictor of patient outcomes,” said Aaron Logan, associate professor, Division of Hematology and Blood and Marrow Transplant, UCSF. “Quantification of MRD should be standard practice to assess response to treatment, monitor disease progression and direct patient care. It is thus essential to have an MRD assay that meets regulatory standards and can accurately and reliably measure and track disease burden over time.”
For patients who achieve complete response to cancer treatment by traditional response criteria, the presence or absence of MRD has been demonstrated to have a significant relationship with patient outcomes.2 For this reason, many pharmaceutical companies have begun using MRD as a clinically meaningful endpoint to evaluate efficacy and to guide use of their therapies.
“This year has been historic for the field of hematology, with a paradigm-shifting FDA decision to approve the first therapy, BLINCYTO, based on the MRD status of a patient with ALL, validating the clinical relevance of MRD in ALL as a clinically meaningful endpoint,” said Greg Friberg, M.D., vice president, Global Development, Oncology at Amgen. “Now, physicians and patients will have access to the first FDA-cleared MRD assay, providing them with another important tool to make informed decisions about treatments to help achieve MRD negativity. We look forward to continuing our collaboration with Adaptive Biotechnologies to further explore MRD and deliver on our mission to serve patients through transformative science.”
The recent FDA review and approval of drugs with MRD included as a clinical endpoint, as well as the agency’s inclusion of MRD on the recently released list of surrogate endpoints that can serve as the basis of drug approvals, demonstrate the clinical actionability of MRD and reinforce the need for an accurate and standardized, FDA-cleared method like clonoSEQ.3,4
“The clearance of the clonoSEQ Assay is an exciting advance for MM and ALL patients and physicians; as MRD is increasingly used to inform treatment decisions, the importance of having an accurate and standardized assessment method becomes paramount,” said Chad Robins, chief executive officer and co-founder of Adaptive Biotechnologies. “NGS MRD testing is already part of National Comprehensive Cancer Network (NCCN) treatment guidelines for patients with MM, ALL, and CLL, and clonoSEQ is already in use for patient management in the majority of NCCN cancer centers, further demonstrating the clinical importance of MRD and acceptance of NGS MRD testing by the oncology community. Adaptive is working diligently with public and private payers to make clonoSEQ broadly available to patients in need.”
About Minimal Residual Disease
Minimal residual disease (MRD), also referred to as measurable residual disease, refers to cancer cells that remain in the body after treatment for patients with lymphoid cancers. These cells can be present at levels undetectable by traditional morphologic methods, microscopic examination of blood, or a bone marrow or a lymph node biopsy.
MRD is used by physicians to detect and monitor disease burden in patients and to inform their treatment decisions. Clinical practice guidelines recommend assessing MRD at multiple time points during treatment and maintenance in MM and ALL, and guidelines for both diseases include NGS as a recommended testing method.5,6 The prognostic value of MRD assessment has been demonstrated in multiple lymphoid cancers.7,8 Controlled trials have shown that even small amounts of disease are profoundly significant for predicting a patient’s long-term clinical outcomes.1,9,10,11,12 Therefore, highly sensitive, standardized molecular technologies are needed for reliable detection of MRD.
Measurement of MRD is currently being evaluated as a way to measure efficacy in drug trials, with the potential to expedite the approval of emerging therapies.13
About the clonoSEQ® Assay
The Adaptive Biotechnologies clonoSEQ Assay has been granted De Novo designation by the FDA as an in vitro diagnostic (IVD) to detect and monitor minimal residual disease (MRD) in patients with multiple myeloma (MM) and B-cell acute lymphoblastic leukemia (ALL) using DNA from bone marrow samples. It identifies and quantifies specific DNA sequences found in malignant cells, allowing clinicians to monitor patients for changes in disease burden during and after treatment. This robust assay provides sensitive and accurate measurement of residual disease that allows physicians to predict patient outcomes, assess response to therapy over time, monitor patients during remission and detect potential relapse. The clonoSEQ Assay is a single-site assay performed at Adaptive Biotechnologies. It is also available as a CLIA-regulated laboratory developed test (LDT) service for use in other lymphoid cancers.
clonoSEQ was reviewed under the FDA’s De Novo premarket review pathway, a regulatory pathway for some low- to moderate-risk novel devices for which there is no legally marketed predicate device.
For important information about the FDA-cleared uses of clonoSEQ, including the full intended use, limitations, and detailed performance characteristics, please visit www.clonoSEQ.com/technical-summary.
About Adaptive Biotechnologies
Adaptive Biotechnologies is the pioneer and leader in combining next-generation sequencing (NGS) and expert bioinformatics to profile T-cell and B-cell receptors. Adaptive is bringing the accuracy and sensitivity of its immunosequencing platform to researchers and clinicians around the world to drive groundbreaking research in cancer and other immune-mediated diseases. Adaptive also translates immunosequencing discoveries into clinical diagnostics and therapeutic development to improve patient care. For more information, please visit adaptivebiotech.com.
Adaptive Biotechnologies does not endorse the use of any particular therapy.
1 Perrot A, et al. Blood. 2018:blood-2018-06-858613.
2 Martinez-Lopez J, et al. Blood. 2014;123(20):3073-9.
3 BLINCYTO (blinatumomab) Full Prescribing Information. Retrieved September 26, 2018 from: https://pi.amgen.com/~/media/amgen/repositorysites/pi-amgen-com/blincyto/blincyto_pi_hcp_english.pdf
4 DARZALEX (daratumumab) Full Prescribing Information. Retrieved September 26, 2018 from: http://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/DARZALEX-pi.pdf
5 NCCN Clinical Practice Guidelines in Oncology for Multiple Myeloma. V.3.2018.
6 NCCN Clinical Practice Guidelines in Oncology: Acute Lymphoblastic Leukemia. Version 1.2018.
7 Wu, D, et al. Clin Cancer Res. 201:20(17):4540-9.
8 Korde N, et al. JAMA Oncol. 2015:1(6):746-54.
9 Dimopoulos MA, et al. N Engl J Med. 2016;375:1319-1331.
10 Pulsipher M, et al. Blood. 2015;125(22):3501-8. Adaptive Biotechnologies provided financial support for this study.
11 Mannis GN, et al. Biol Blood Marrow Transplant. 2016;22:1030-1036. Adaptive Biotechnologies provided financial support for this study.
12 Logan AC, et al. Biol Blood Marrow Transplant. 2014;20(9):1307-13. Adaptive Biotechnologies provided financial support for this study. Clinician has received compensation to participate in advisory meetings sponsored by Adaptive.
13 Avet-Loiseau H. Am Soc Clin Oncol Educ Book. 2016; 35e425-30.
View source version on businesswire.com: https://www.businesswire.com/news/home/20180928005655/en/
Contacts
Adaptive Biotechnologies
Beth Keshishian, 917-912-7195
media@adaptivebiotech.com